Category
Research
Ultrasound
Year
2026
Market
Hospitals
Detecting elevated intracranial pressure non-invasively at the bedside has long been a goal of acute care medicine. Optic nerve sheath diameter (ONSD) ultrasound offers a practical solution and the evidence base to support it.
The optic nerve is surrounded by a meningeal sheath that is continuous with the intracranial subarachnoid space. When intracranial pressure (ICP) rises, that pressure transmits along the sheath, causing it to distend. Using a high-frequency linear transducer placed gently over the closed eyelid, we can measure that distension in real time; non-invasively, without radiation, and repeatedly at the bedside.
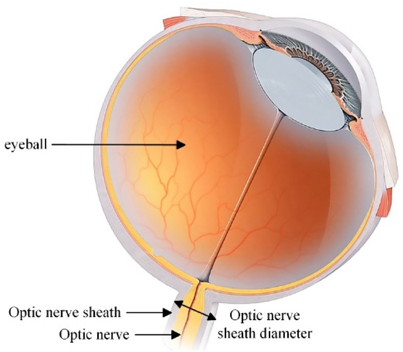
The standard technique uses a linear probe (~7.5 MHz ) with the patient supine. The sheath is measured 3 mm posterior to the globe, perpendicular to the optic nerve axis, with multiple measurements taken across both eyes and averaged. A diameter above approximately 5.0 mm is the most widely supported threshold for elevated ICP; however, should be thought of as a continuous spectrum as different thresholds have been studied in the literature.
Ultrasound is particularly valuable for estimating ICP during acute, austere, remote, and field scenarios. Unlike CT or MRI, it requires no specialist infrastructure, produces no radiation, and can be performed repeatedly anywhere, by a trained provider. This makes it viable not just for a single diagnostic decision, but for serial monitoring and evolution of brain injury.

Across multiple systematic reviews and meta-analyses, the diagnostic performance is consistent: Koziarz et al. (2019) reported 97% sensitivity and 86% specificity in TBI populations across 71 studies and 4,551 patients, with an optimal threshold of approximately 5.0 mm. Robba et al. (2018) found a pooled diagnostic odds ratio of 67.5 and HSROC AUC of 0.938. Kim et al. (2019) reported 99% sensitivity at the same threshold. The signal across all reviews is clear: ONSD helps rule out elevated ICP when normal, and when increased, raises concerns for elevated ICP.
ONSD ultrasound is a plausible and evidence-supported adjunctive neurodiagnostic tool for acute care medicine. Its strengths align closely with the demands of bedside practice: portable, non-invasive, repeatable, and capable of providing a meaningful physiologic signal when advanced imaging and specialist consultation are unavailable.



