Category
Education
Year
2026
Market
Defense
Biological inhalational threats produce distinct and clinically meaningful pulmonary findings; and lung ultrasound is well positioned to detect them. While the sonographic presentations vary across agent classes, the common thread is that ultrasound provides early, actionable physiologic information at the point of care, before definitive agent confirmation is available and before casualties have necessarily declared clinical deterioration. This post covers the expected ultrasound patterns for the three key biological inhalational threat categories and how those findings support frontline decision-making.
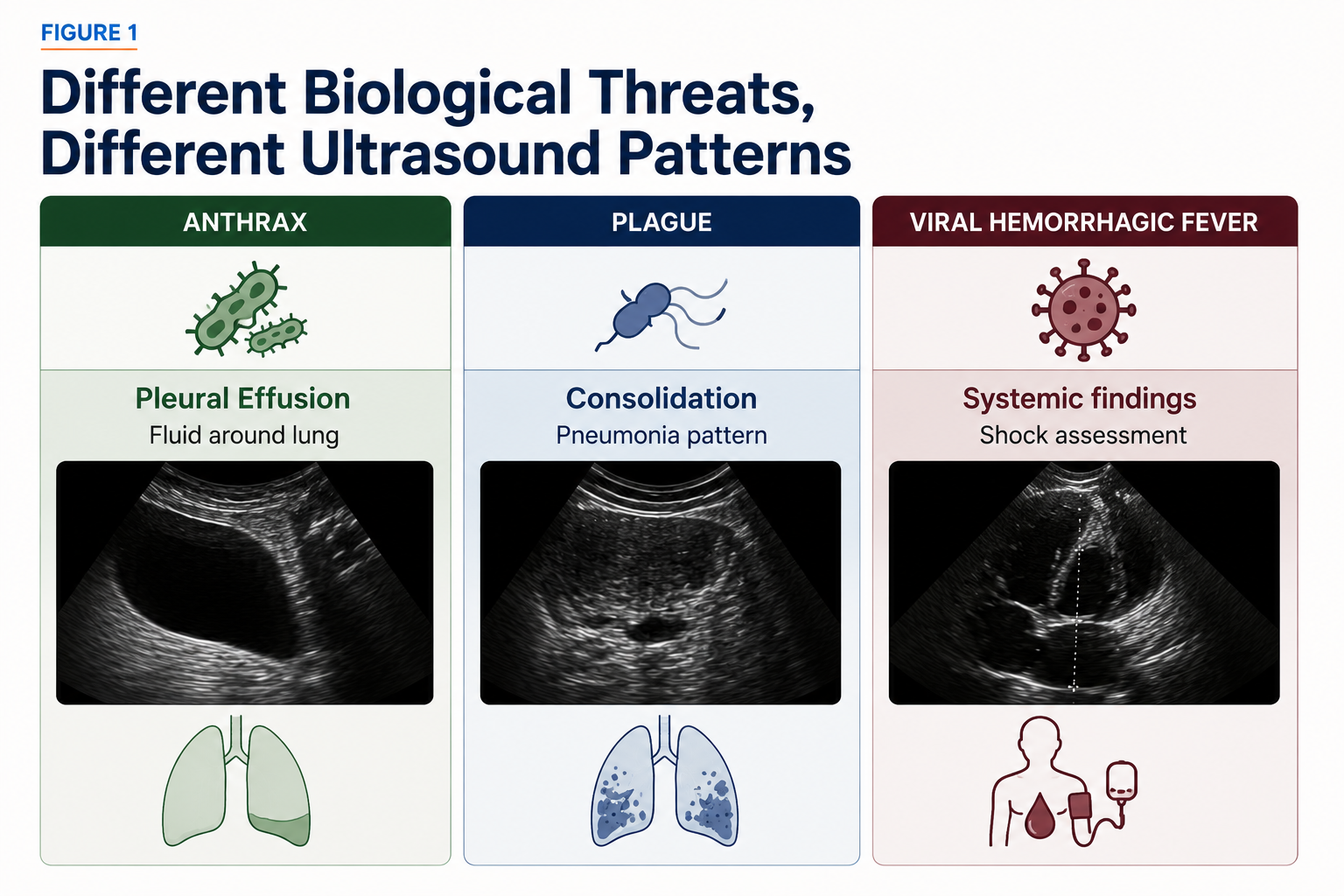
Inhalational anthrax
Inhalational anthrax has a well-characterised imaging phenotype, and lung ultrasound plays a focused role within it. The signature finding is bilateral pleural effusion; often large, and potentially complex or echogenic due to the haemorrhagic nature of anthrax-related effusions. Chest X-ray or CT imaging remains essential for a complete evaluation when anthrax is suspected.
Pneumonic plague
Pneumonic plague is a severe respiratory infection that typically appears on lung ultrasound as areas of lung consolidation rather than diffuse B-lines. Because the disease can progress rapidly, serial ultrasound examinations may help clinicians track worsening lung involvement over time. While ultrasound cannot diagnose plague itself, it can help identify a rapidly progressing pneumonia pattern and support timely treatment, isolation, and triage decisions.
Viral hemorrhagic fevers and systemic biological illness
For diseases such as Ebola, Marburg, and Lassa fever, ultrasound is often more useful for assessing the body's overall condition than for detecting lung injury. Clinicians can use ultrasound to evaluate shock, fluid accumulation, or cardiac complications, while lung findings tend to be nonspecific or appear later in the disease course.
Across all three biological threat categories, a consistent operational advantage emerges: lung ultrasound delivers physiologic information earlier than conventional imaging, at the point of care, and with no ionising radiation.
Serial examination amplifies that advantage. A casualty who is reassuringly stable on first scan but developing bilateral effusions or spreading consolidation on the second has declared their trajectory. That trajectory data, captured at the bedside, in real time, is what drives earlier, better-calibrated triage decisions: who gets escalated, who gets evacuated, who gets antibiotics or respiratory support first.

Figures were created specifically for this article series using original illustrations and AI-assisted graphic design tools. Clinical concepts were derived from the references cited in the accompanying text.
1. Earls JP, Cerva D Jr, Berman E, et al. Inhalational anthrax after bioterrorism exposure: spectrum of imaging findings in two surviving patients. Radiology. 2002;222(2):305–312.
2. Wang W, Li X, Wu J, Fu X, Li B. Imaging analysis of pneumonic plague infection in Xizang, China: a case report and literature review. BMC Pulm Med. 2024;24(1):1–6.
3. Lichtenstein D, Meziere G, Biderman P, Gepner A, Barre O. The comet-tail artifact: an ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med. 1997;156(5):1640–1646.
4. Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577–591.
5. Baloescu C, Moore CL, Wyer PC, et al. Artificial intelligence guidance of lung ultrasound by trained nonexperts. JAMA Cardiol. 2025;10(3):234–241.


