Category
Education
Research
Ultrasound
Year
2026
Market
Defense
Chemical, biological, radiological, and nuclear (CBRN) inhalational exposures present one of the most complex triage challenges in military medicine and mass-casualty response. Clinical examination is degraded by personal protective equipment (PPE), radiological imaging is often unavailable forward of higher-echelon care, and agent confirmation can be significantly delayed. In this environment, lung ultrasound offers an attractive solution for early detection and monitoring of pulmonary injury as a portable, repeatable, non-ionizing point-of-care imaging modality.
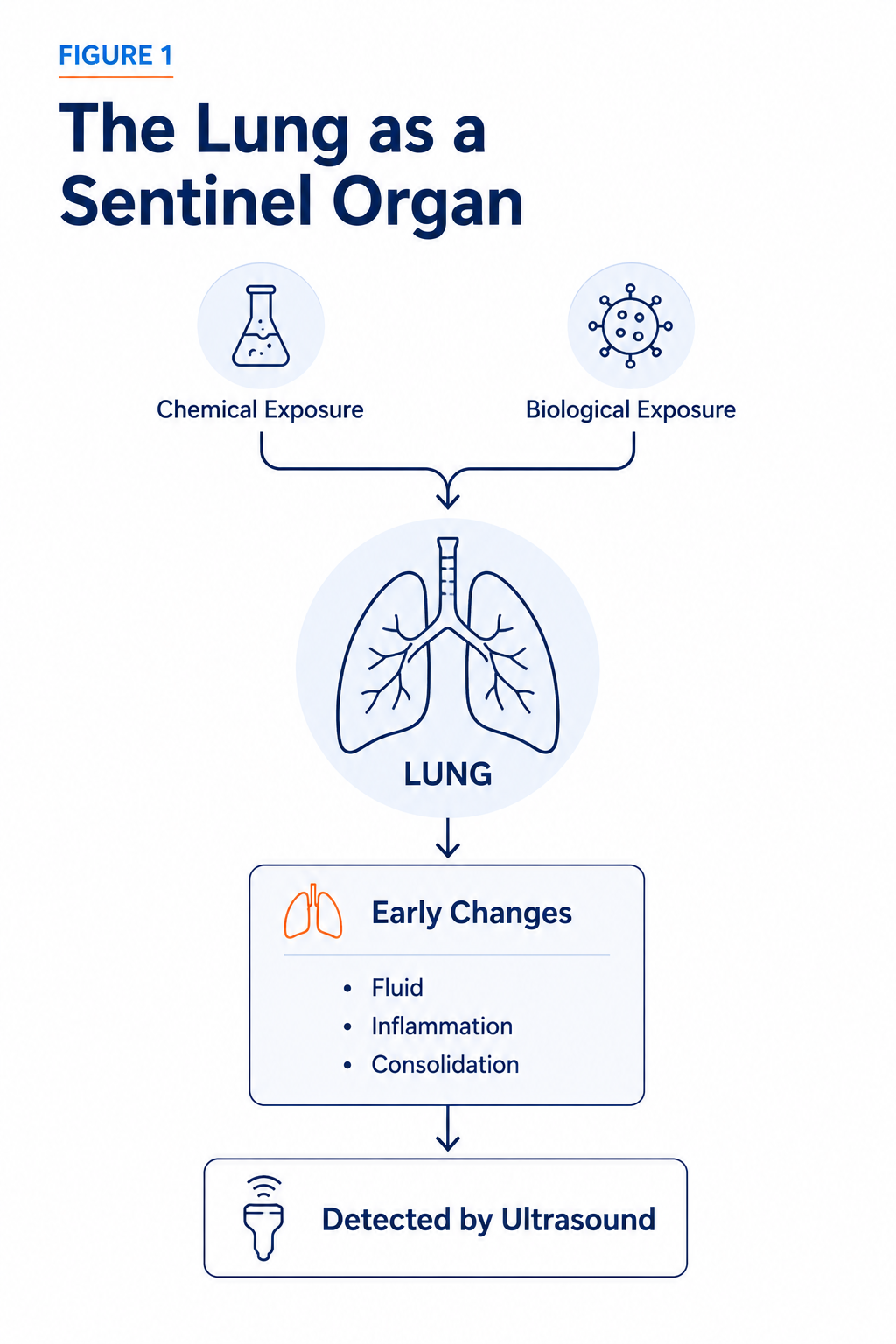
The lung is often one of the first organs to show signs of injury following exposure to inhalational chemical or biological threats. Despite differences in how these agents cause harm, many produce similar pulmonary effects (such as fluid accumulation, interstitial thickening, consolidation, and respiratory failure) that can be detected with lung ultrasound. This makes the lung a valuable "sentinel organ," providing early insight into downstream injury and helping clinicians identify evolving respiratory pathology when rapid assessment is critical.
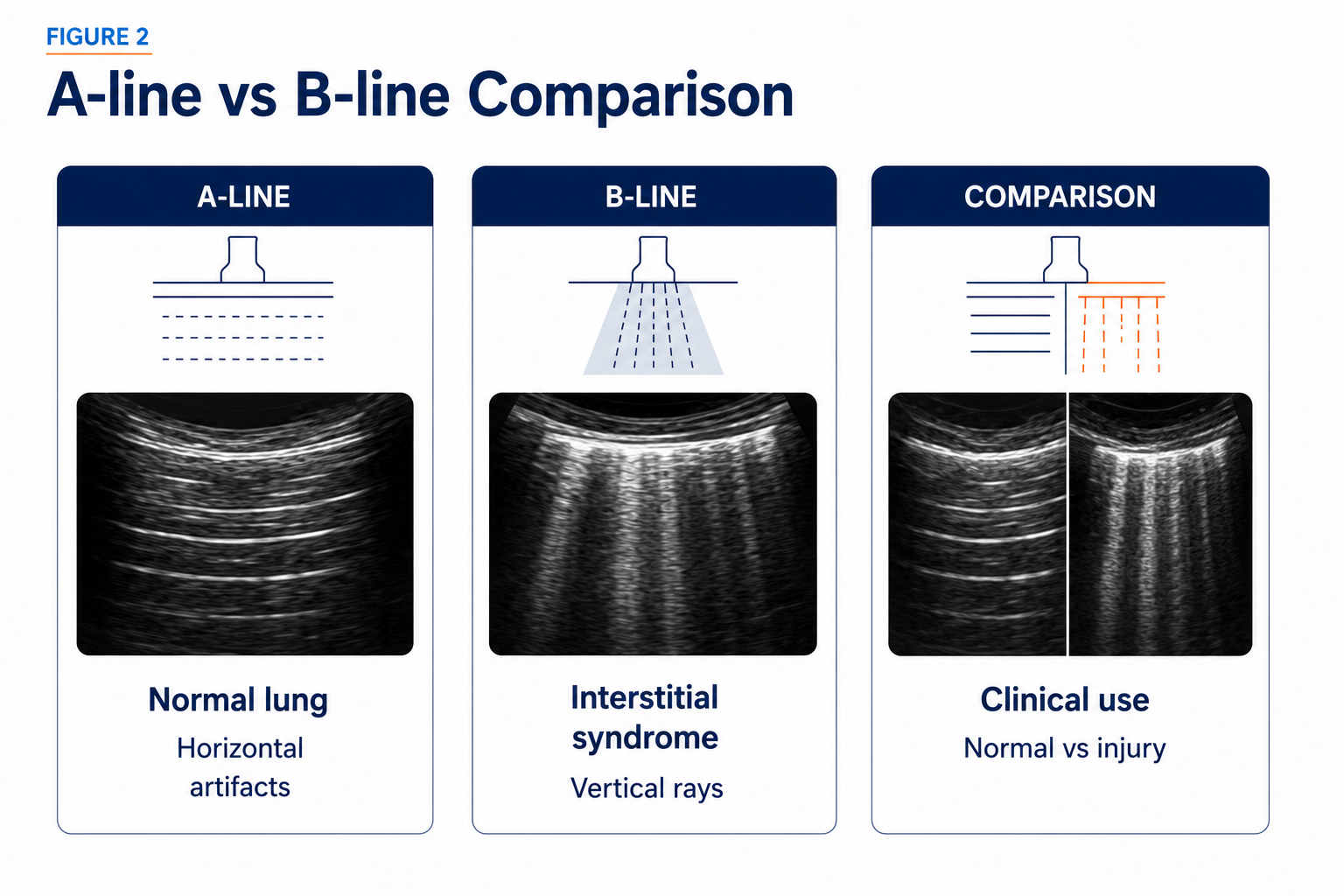
Lung ultrasound patterns can provide important clues about respiratory injury. A-lines are associated with normal, well-aerated lung tissue, while B-lines may indicate increased lung fluid, inflammation, or other forms of alveolar-interstitial injury. Rather than relying on B -lines alone, clinicians assess a broader ultrasound phenotype that includes pleural abnormalities, consolidations, effusions, and lung sliding. Together, these findings help characterize the severity and nature of pulmonary injury, supporting the evaluation of conditions ranging from toxic inhalation to severe respiratory infections.
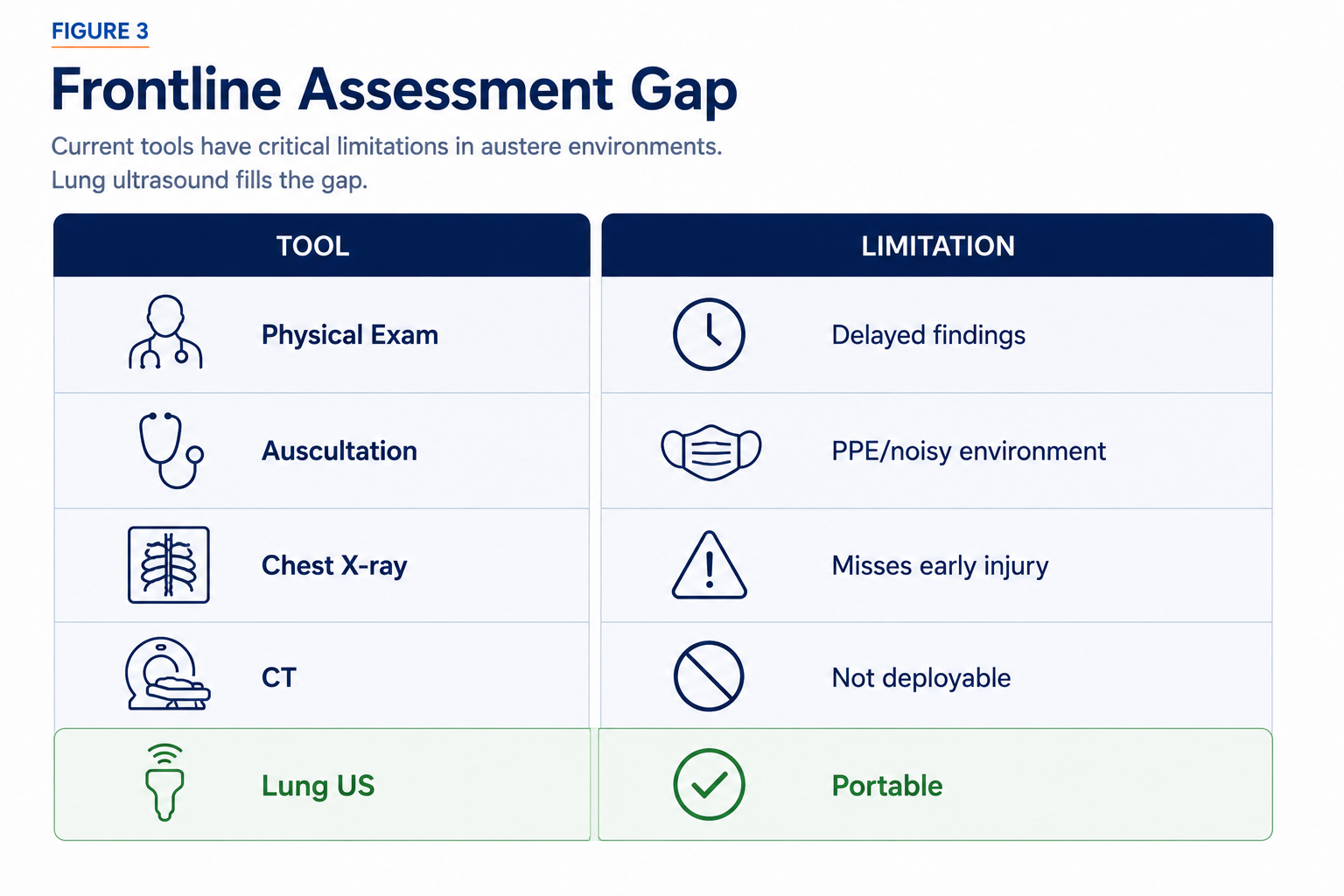
Frontline assessment of respiratory injury relies heavily on clinical examination, chest X-ray, and CT imaging, but each approach has limitations. Clinical signs may not appear until injury has progressed, while auscultation can be unreliable in noisy environments or when providers are wearing personal protective equipment. Chest X-rays may miss early lung injury, and although CT provides detailed imaging, it is often impractical in prehospital, contaminated, or mass-casualty settings. These challenges highlight the need for rapid, portable tools that can help identify pulmonary injury earlier and closer to the point of care.
While lung ultrasound is not a standalone diagnostic tool for chemical or biological exposure, it has significant potential as a frontline aid for pulmonary assessment. In operational environments where timely triage and resource allocation are critical, lung ultrasound is a valuable addition to chemical and biological exposure response protocols.

Figures were created specifically for this article series using original illustrations and AI-assisted graphic design tools. Clinical concepts were derived from the references cited in the accompanying text.
1. Lichtenstein D, Meziere G, Biderman P, Gepner A, Barre O. The comet-tail artifact: an ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med. 1997;156(5):1640–1646.
2. Jambrik Z, Gargani L, Adamicza A, et al. B-lines quantify the lung water content: a lung ultrasound versus lung gravimetry study in acute lung injury. Ultrasound Med Biol. 2010;36(12):2004–2010.
3. Torino C, Gargani L, Sicari R, et al. The agreement between auscultation and lung ultrasound in hemodialysis patients: the LUST Study. Clin J Am Soc Nephrol. 2016;11(11):2005–2011.
4. Soldati G, Testa A, Silva FR, Carbone L, Portale G, Silveri NG. Chest ultrasonography in lung contusion. Chest. 2006;130(2):533–538.
5. Baloescu C, Moore CL, Wyer PC, et al. Artificial intelligence guidance of lung ultrasound by trained nonexperts. JAMA Cardiol. 2025;10(3):234–241.
6. Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577–591.